Every time I wrote this past 9 months, I found myself acknowledging yet another looming natural tragedy (wildfires, hurricanes) or the many man-made tragedies.
I embrace and rally behind the idea of ceremonial hurricane flag burning, which those in Florida Keys do yearly (you can find videos of it – they did it yesterday to mark the end of hurricane season, the worst on record, I believe).
I hope to one day have a ceremonial burning of that COVID-19 red cell image we are now so numb to seeing.
We are entering into a new season and with COVID-19 infections increasing in most areas. We had some warmer months to figure out some things (e.g., accessing PPE; sorting out safety protocols; equipping vehicles for safer transport; figuring out a balance of using telehealth vs in-person visits; creating partnerships for food delivery services; getting to know long lost Aunt Charlotte to step up with more support of her nephew; finding out they really can do quite well managing their meds with less frequent med deliveries; helping them access and use new phones).
But, to quote one of my favorite series, Winter is Coming. We will have new challenges with all the states and provinces operating in colder temps. Outdoor visits will likely be shorter or less agreeable. If we don’t get aid packages out for all, demand for limited supplies will only increase and resources more stretched.
Creativity and leadership will be paramount. Attention to providing right-level supports for people in meaningful ways will also remain critical.
So, without further pontification and babbling, here are a list of resources to consider (all FREE).
Third, wanted to remind you of this resource: https://smiadviser.org/ There is a Clozaril consultation clinic embedded within, and they host virtual consultations (next one tomorrow afternoon). We have heard psychiatric care providers finding it to be very valuable. Check out their calendar for quickest view of live events, but they also have a huge catalogue of recorded webinars, too.
Lastly, we continue to host National ACT Meet-Up Calls. We host a monthly meeting the first Monday of the month (next one this coming Monday) for all ACT stakeholders (primarily providers, governing authorities, funders, TA staff, researchers). You can register for the whole series here: https://attendee.gotowebinar.com/register/5320551466410710029
We appreciate you all – as we often find ourselves saying, “this was already hard work before COVID-19… but not surprisingly, the MacGyver-like ingenuity of ACT team members is shining through in how you are addressing these new challenges.
We asked about your own efforts to assess (via standardized measures) “adulting” (functioning, independence, etc). I asked specifically about those using the DLA-20, and how functional assessments themselves vary in their intent (e.g., is it to understand right level of service fit; or to actually gather information to guide how to best target service supports and interventions?). We received 29 responses, representing 12 states. Most everyone reported “yes” to the question: “Do you use any assessment tool to assess adulting/community participation/functioning?” Of my “yes” respondents, a handful indicated that the functional assessment was embedded in a much larger assessment and was limited in scope and depth (i.e., not tremendously useful).
Eight (8) respondents indicated that they complete the DLA-20, and most indicated that it served to guide interventions and supports more than it served to determine the right level of service (i.e., ACT or something else). Most were completing /updating the DLA-20 quarterly and that it took an experienced user 10-15 minutes to complete for follow-ups (the initial can take much longer). DLA-20 users varied in how useful they found it (sometimes critiquing that it is not fully used in the way it could be; questioning who should be primary source of data (client self-report; team member evaluation and judgement); challenge in capturing real change and impact given common fluctuations among people with serious mental illness — hard to fully see positive impact over time when looking at status every 90 days).
I wanted to pass on other assessments people reported to be using and with positive endorsements:
Another shared they did not like the current tool and they are shifting to the Reaching Recovery out of the Mental Health Center of Denver: https://mhcd.org/reaching-recovery-home/
Another shared they continue to rely on assessment tools in the NAMI ACT Start-Up manual, commenting: ” each assessment used is completed with a strengths/needs and recommendation portion for future goal development.”
Sounds like there are options out there — and room for even better options to emerge. We will continue to follow-up on this (and don’t forget we have a Discussion Forum!!! A great place to follow a thread/contribute to a conversation). Wishing that you had contributed your thoughts and ideas? You still can here: https://www.surveymonkey.com/r/ADULTINGassessmnt
An update has been posted today and shared with all TMACT users across the US and abroad, as well as posted on our website (where you can download the TMACT).
When developing the TMACT, we omitted DACTS’ items that addressed features of the team that were not necessarily defining of ACT program fidelity, albeit likely influential on overall program fidelity. These included two DACTS items: Continuity of Staffing (H5) and Staff Capacity (H6). Despite our excluding these two items, we came to incorporate into the protocol rating rules intended to avoid penalizing teams for periodic, unavoidable staff turnover.
Applied solely to the Specialist Team (ST) subscale, if the specialist position (i.e., ST1, ST4, ST7) was newly filled or recently vacated, we included an option to not rate them on the subsequent performance items (i.e., ST2 and ST3; ST5 and ST6; ST8). The following is a rating guideline example from ST1 (p.68, Part II):
“NOTE: If there is no COD specialist on the team, rate this item as a “1,” but do not rate ST2 and ST3 if COD specialist vacancy has been less than 6 months. Also, rate COD specialists hired within past two months on this item, which will likely be a low rating as they likely are not yet operating fully within their specialty role, but do not rate on ST2 and ST3. If hired more than two months before review, rate new specialist on ST2 and ST3.”
We have observed that the conditions, as listed, are exceedingly forgiving of teams that experience excessive staff turnover, which was not our intention and compromises the scale’s validity. As such, we are enacting the following update, which observes the intention of the DACTS while also continuing to observe our aim to not penalize teams for natural, periodic staff turnover:
“NOTE: There is an option to skip the subsequent ratings for the “In Treatment” and “Within Team” performance items if this position is vacant for a short period, or if recently filled with a new employee. To qualify for this option, the following conditions must be met:
The position of interest has been vacant fewer than 4 months, or
The position of interest has been newly filled for fewer than 2 months, AND
The team has not experienced excessive staff turnover, as indicated by the team rating a 4 or 5 on the DACTS’ H5 Staff Turnover Item, which reflects an annual staff turnover rate of 39% or less.
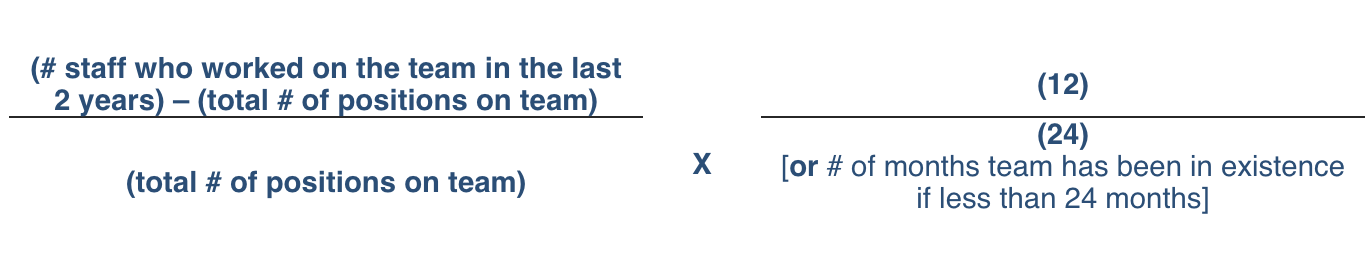
To calculate an average annual staff turnover rate:
Refer to the Team Survey #2. The team reports the # of staff who have left the team within the past 2 years (or update if shorter time frame of team operation).
Determine the total # of positions on the team. Add up the positions listed in the Staffing Table (Item #1), and add in vacant positions. A single part-time position = one position. Two part-time positions = two positions.
Calculate an Annual Staff Turnover Rate using the below formula (multiply by 100 to get a percentage).
This 2 1/2-day in-person training accompanied with pre-recorded webinars covers ACT topics, including: ACT History, Research, and Fidelity; ACT Staffing; ACT Leadership: ACT Medical Team; ACT specialists and related specialty services (co-occurring substance use, employment, peer support, housing, psychiatric rehabilitation); assertive outreach; assessment and person-centered planning; and daily team meeting.
Training is led by UNC Institute for Best Practice staff, Lorna Moser, Ph.D. and Stacy Smith, MEd, LPC, MINT Member, as well as guest speakers. Training is appropriate for both new ACT providers, seasoned ACT providers, and other stakeholder groups (e.g, ACT governing bodies and MCO staff). Participation meets requirements of NC DHHS ACT Policy for new ACT team members. Out-of-state attendees welcome.
A Wisconsin colleague and friend had posed a question to the listserv last month, of which 20 of you provided some responses (thank you!). The essence of the question was — do you have access to a specialized psychiatric crisis response center and/or do you interface with a general hospital’s crisis center. Related questions sought to understand the good and the bad of each (e.g., we continue to move towards more integrated care and does specializing and isolating behavioral health/psychiatric crisis services undercut that effort? Or, are the needs so unique that having specialized psychiatric crisis services is really best care and coordination).
11 of you indicated that you only access emergency depts within general hospitals.
3 of you indicated that you only access specialized psych emergency depts/crisis stabilization units
6 of you indicated that you have access to both.
Below are some questions and responses:
Does your area have problems with extensive emergency room department “boarding” – where the individual may sit for hours, even days, to access a bed and services? 16 (80%) responded YES. Some clarified that it may be hours. Here are some specific responses (with notation if they said general hospital, psych ED, or both above):
“Most all state hospitals in VA are over capacity following trickle down effects of “Bed of Last Resort”/Creigh Deeds incident. Local, private hospitals deny admission for people that are aggressive, highly psychotic, etc. essentially sending them to state hospitals since they cannot deny admission. It has created huge problems within the VA system which feels like it is nearing a breaking point. ACT teams cannot get individuals hospitalized locally and if they do make it in the door and do not clear within a couple of weeks, they are generally discharged because there are no transfers to longer term care anymore. Folks that are TDO’d for acute hospitalization are sitting in ER’s for days now waiting on a bed somewhere in the state.” (BOTH)
“Our most recent experience involved a 22 year old held in the emergency room from Friday to Monday, then sent from (central Minnesota) to ND. Put on 72 hour hold prior to transport, discharged after 2 days. We scrambled for placement. From there he went to an IRTS (very south-western MN). That was a 16 hour trip to transport him.” (BOTH)
“Finding a bed for someone with significant psychosis AND physical health issues in the local area is impossible. They have to go outside of our community.” (BOTH)
“Often clients can wait several hours to be seen by the Behavioral Health team at the hospital. If there is not a bed available on the Behavioral Health Unit they will be transferred to another hospital. This process could take upwards of 24-36 hours. During this time clients will become agitated, desire to leave, or become involuntarily hospitalized.” (General Hospital – but recently started a Crisis Intervention Team Assessment Center within the local hospital)
“The individual may sit for hours before being transported to the Psych “department” for that hospital; the other hospital is usually full and will keep individuals on a Psych hold in the general ER. The hold in the ER can last for days.” (Gen Hosp)
“Clients will sit in holding for days waiting on a bed, and sometimes client get sent to hospitals quickly that don’t require an assessment but they don’t typically get the best care at those hospitals.” (Gen Hosp)
“Many patients board regularly in the psych Ed while awaiting inpatient beds and or transfers within county to psych beds particularly in the weekend” (Psych ED)
“The certified pre-screener is responsible for typing up the assessment and collecting medical clearance. Sometimes medical clearance takes a long time if the client cannot pass urine or refuses labs. Both medical clearance and prescreen assessment are needed to start a bed search. The length of time to call each hospital, fax and follow up to see if the fax was reviewed can be extremely lengthy.” – ps this is in VA, similar to the first response above. (BOTH)
“Hours, not necessarily days.” (BOTH)
“rarely, but it does happen. not for days, but to sit for a few hours waiting to get responses from hospitals for admission is common.” (Gen Hosp)
If you have access to a specialized psychiatric
emergency department, or crisis stabilization unit, what has been helpful about
how this has been designed? Anything not so helpful (that could be
better)?
“We have one regional Crisis Stabilization unit in our region (city of Richmond and surrounding counties) and they have provided excellent treatment, in many cases better than acute hospitalization with the requirement of active treatment vs being housed in a local hospital bed until the acute crisis passes. They are also somewhat selective in who they accept and they are very reluctant to admit someone unless they have housing already in place or firmly lined up prior to admission.”
“There is a Crisis Unit in (MN). We have to ensure that the individual brings their own meds and they will not prescribe/change medication. Not changing the medication is a positive in cases where the individual was not taking meds.”
“Currently we just had a CITAC (Crisis Intervention Team Assessment Center) open at our local hospital. If someone is brought to the ED by police for evaluation they are met by a peer support, trained law enforcement, and mental health clinicians who support the client through the process. It has only been open a couple of months but we hope to see a positive impact with it.”
“It is helpful that we don’t always have to go through the hospital to do an admit if needed and we can just do a direct admit to the CSU.” (CSU- crisis stabilization unit)
“The referral form is the pre-screening form, in the event they escalate to the level of need of a TDO (I think temporary detention order – Lorna) we are able to do this quite quickly.”
“We have access to state and privately ran crisis/triage hospitals and stabilization units. It is most certainly easier on the clients to be in a facility that specializes in behavioral health. The teams also develop great working relationships with consistent staff on the specialty units. Those relationships have become tremendously helpful when collaborating during a hospitalization. Utilizing emergency departments was a procedure many many years ago and would, unfortunately, feel like going backwards if it were to occur in our area. The facility that accepts mainly Medicaid has a unit with “23 hour beds”. This becomes mainly an acute stabilization and if further care is needed, they will go to a “bed” on the longer term unit. We have a variety of resources, however, we still feel short of beds frequently. When beds not available in our county, they will be driven, by sheriff deputies, to other county agencies in the state for treatment.”
Where did our respondents come from? Virginia, Minnesota,
Oklahoma, New York, North Carolina, Indiana, Florida, George, and Colorado
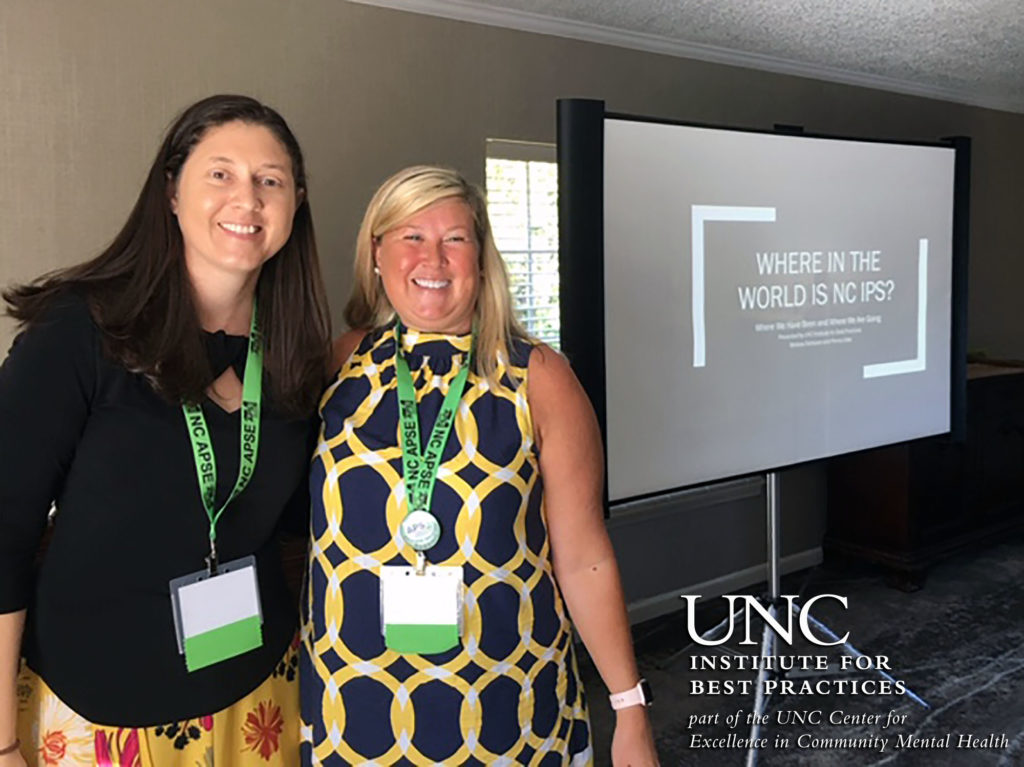
The Institute’s Penny Liles & Melissa DeHaven presented on IPS Fidelity at the recent NC APSE Conference in Blowing Rock. Trends in the state’s 5 years of data were compared to the IPS Learning Collaborative’s larger data set.
In the afternoon, Melissa & Penny continued by speaking on Assertive Engagement strategies.
Here in the U.S., we are once again reeling from a series of mass shootings and the unavoidable aftermath of debates and inaction. Harvey Rosenthal—the CEO of the New York Association of Psychiatric Rehabilitation Services and a staunch advocate for people with mental illness—wrote this opinion piece, published in USA Today yesterday, titled, “I have a mental illness. Don’t scapegoat, institutionalize people like me after shootings.”
Why share this
particular piece of the many that are out there?
Because the discourse again has gone the direction of finger-pointing towards mental illness with proposed “solutions” involving coercion and control. I suspect there are some people, including people getting ACT services, who could benefit from open discussion and processing following the events themselves, but also the de facto finger-pointing. For many individuals getting ACT, we are their biggest advocate and it may be times like this when our advocacy needs to be the loudest.
The Individual Placement and Support (IPS) 101 training formerly called SE Foundations is required by all IPS team members (Team Lead, Employment Specialist, and Employment Peer Mentor) and Assertive Community Treatment team members (Vocational Specialists and Team Leaders).
The two-day training will be an introduction to the evidence-based practice, incorporating the philosophy, practice principles, and the elements of the practice.
Peer Specialists are particularly underpaid and have a limited career growth trajectory within the “peer specialist” position. We’ve seen peers continue to invest in their own career development, furthering their education and training, and eventually moving into other ACT team positions or out of ACT all together. When they do move into the other positions, with their more advanced education in hand, they then get access to a salary boost. Whatever position they land in, they (hopefully) never lose their “peerness” and integrate that within the other position.”Peerness,” to me, is navigating the role of being part of a larger team of professionals, while aligning closely to the people served, helping serve as their voice within the team and larger system, while also teaching individuals the skills to be their own advocate. Peers carry an anchor of empathy – not only from the experience of struggling with mental illness (and/or substance use), it’s from being oppressed, overpowered, beaten down.
I get concerned when I see peers embracing or wanting a more “clinical” status — as it may reflect a drift from what is most sacred about their position. On the other hand, I think we create reason for this drift because we continue to undervalue this important position, both in fair compensation and career growth options.
A final thought, too, is that I hate how much we separate out peers from other team members who have not self-identified as such. All the unique qualities a peer brings are things we should all be striving to represent and offer to people we serve (advocacy, empathy, patience, broadened perspectives).